Glue ear, grommets, and adenoids
Information for parents from the Ear Nose and Throat (ENT) Department
Your child has been diagnosed as having a problem with fluid or mucus build-up behind their ear drum. This condition is often called “glue ear”. This leaflet explains the following.
How a normal ear and hearing works.
What glue ear and adenoids are.
What causes glue ear, and what the symptoms are.
What treatment is available.
What happens during and after surgery.
We hope this leaflet answers some of the questions you may have. If you have any further questions or concerns, please speak to a member of your child's healthcare team.
How does a normal ear and hearing work?
The normal ear is divided into three parts - outer, middle, and inner ear.
The outer ear funnels sound waves in the air to the eardrum, which forms the boundary between the outer and middle ear. The eardrum vibrates when sounds arrive. The vibrations are transmitted to the inner ear via three small bones (ossicles) suspended in the middle ear.
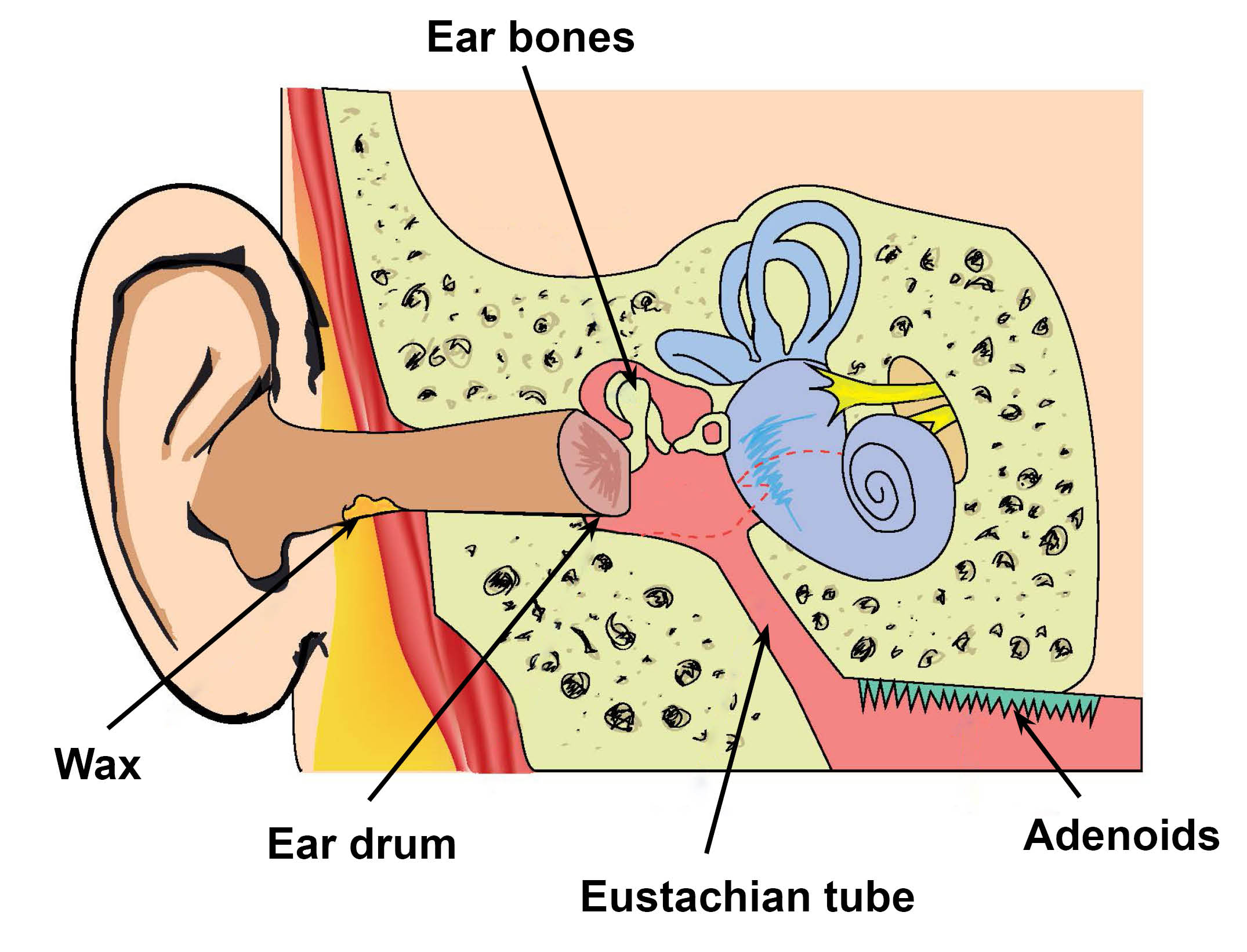
The inner ear acts like a microphone. It turns sound vibrations into electrical signals, which are sent to the brain via the nerve of the hearing. The inner ear is also concerned with balance. To hear normally, the eardrum and ossicles must be able to move easily.
For this to happen the middle ear must contain air at the same atmospheric pressure as the outer ear. The air in the middle comes from the back of the nose via the Eustachian tube.
What is glue ear?
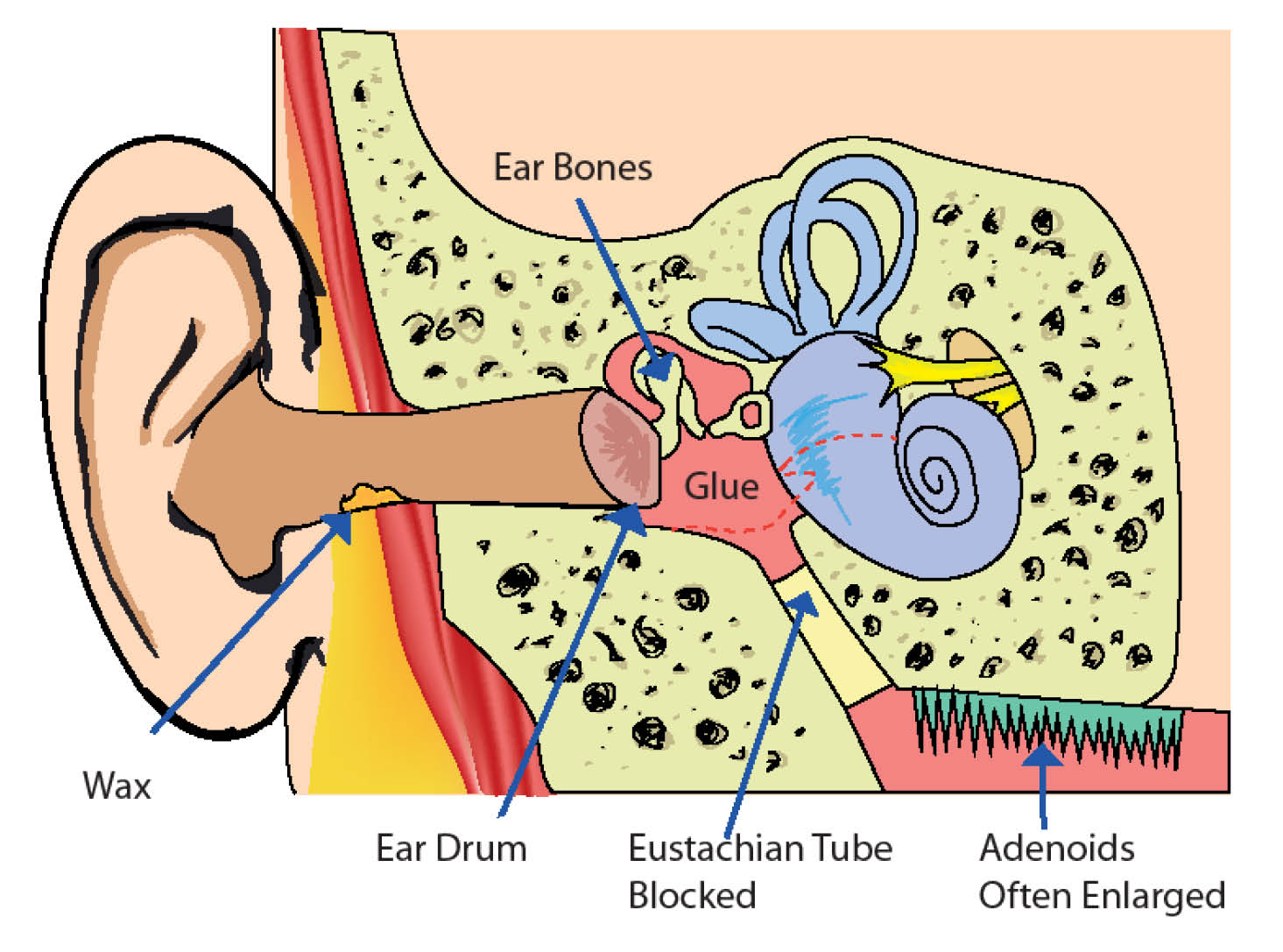
Glue ear is a build-up of fluid behind the eardrum in the middle ear. The fluid may be thick and sticky or thin and watery. Both stop the eardrum and ossicles vibrating easily, so quieter sounds are not heard.
Glue ear is the most common cause of deafness in children. Other names for glue ear are:
middle ear effusion; and
chronic secretory otitis media.
What causes glue ear?
Most children get glue ear after a cold or ear infection. The Eustachian tube is small and blocks easily. It then fails to ventilate the middle ear. Sticky secretions cannot drain away, so fluid builds up in the middle ear. Movement of the eardrum and ossicles is weakened or damaged, causing partial deafness.
Most cases get better quickly after a cold. A small number continue for months or years.
The most common reasons for glue ear to continue are:
large adenoids at the back of the nose; and
passive smoking (inhaling smoke from other peoples’ cigarettes / cigars).
Sometimes glue ear runs in families, although it is not strictly speaking hereditary. Often no cause is found.
What are adenoids?
Adenoids are cauliflower-like swellings of immune tissue at the back of the nose. Normal adenoids help fight off infections. If they get too big they cause blockage of the nose and Eustachian tube. In severe cases they can obstruct breathing at night.
What are the symptoms of glue ear?
Mild to moderate deafness is the most common symptom. It often varies from week-to-week, being worse after a cold.
If deafness happens early in childhood, speech may be delayed. Unclear speech and constant shouting are common.
Education may be affected, as deafness is not always suspected. A child is thought to be inattentive, slow, or lazy, concentration may be poor, and the child often seems to be ‘in their own world’.
Some sufferers get regular earaches and repeated ear infections with high temperatures.
They may also have poor balance and be clumsy.
Older children often complain of noises in their ears.
What are the treatment options?
The fluid can go away by itself, so ‘watching and waiting’ may be best. By the age of 8 years many children have ‘grown out of it’, though this is only the average age. Some will carry on having trouble into their teens. Any factors that make the condition worse should be eliminated, especially passive smoking.
Antibiotics and painkillers, for example Calpol, can be used for ear infections.
Decongestants are often prescribed, but have not been proven to work well.
Glue ear can be seasonal (worse in the winter and better in the summer). Any decision to operate may be delayed if your child is seen in the spring. An operation is more likely to be recommended in the autumn.
The decision to operate is always based on the individual child. For immediate relief, myringotomy and grommet insertion works well. We may suggest removing your child’s adenoids if:
they are enlarged; and
glue ear comes back after the grommets have been inserted.
What is a grommet and how does it work?
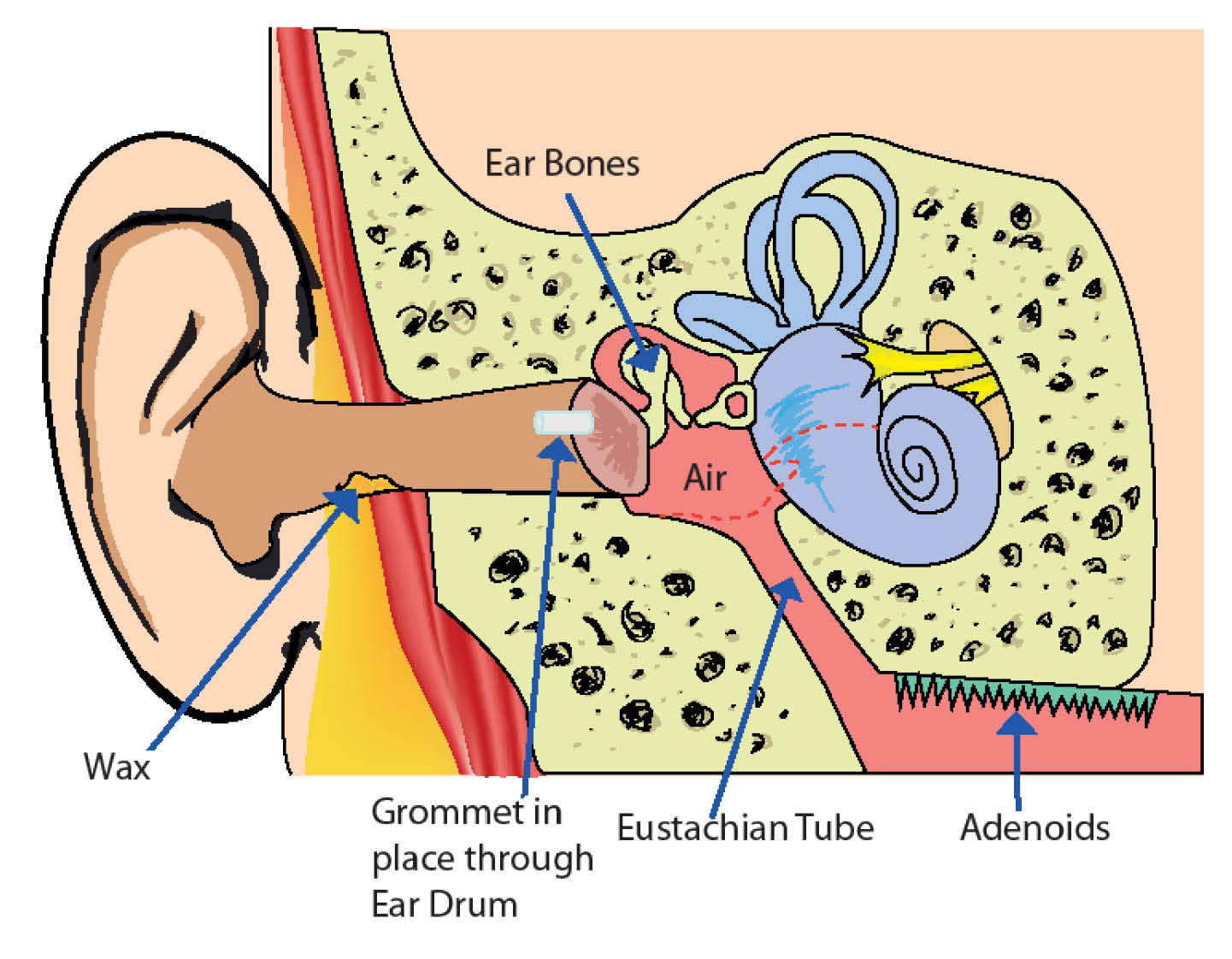
A grommet is a tiny plastic tube, shaped like a mini cotton reel, about 2mm across.
It is fitted through a small cut in the eardrum (myringotomy). The tension of the eardrum grips the grommet. The cotton reel shape prevents it falling in or out.
The grommet allows air from the outer ear directly into the middle ear. If the grommet remains in position and is not blocked, your child’s hearing will return to normal almost immediately. The grommet does not drain fluid out, it lets air into the middle ear.
The grommet is designed to stay in position for about 9 to 15 months. At this point, the eardrum heals over and the grommet drops out.
It is important to understand that a grommet does not cure the underlying cause of glue ear. While it is in position and working, the grommet does give highly effective and immediate relief of deafness and earaches. This buys time, and allows your child the chance to ‘grow out of it’.
If factors such as passive smoking are not dealt with, there is an increased risk that your child’s glue ear will come back once their grommets fall out.
How is the operation done?
Grommet insertion is a quick and simple day case procedure.
It is very delicate and normally done under general anaesthetic (your child will be asleep). The anaesthetic is usually given by injection into a vein in the back of your child’s hand. To stop the needle from hurting, a local anaesthetic cream is usually applied first.
A microscope is used to give a magnified view of your child’s eardrum. A small cut is made in their eardrum and the fluid in their middle ear is sucked out. The grommet is inserted and some ear drops given.
If your child’s adenoids are removed as well, this is normally done under the same anaesthetic. The adenoids are removed through your child’s mouth. No external cut is needed.
Are there any risks?
Every operation carries some risk of infection and bleeding but the hole in the eardrum is tiny, so this risk is reduced. We will give your child a course of antibiotic eardrops to reduce the risk of infection further.
Around 1 in every 100 children may develop a perforated eardrum. If this continues, we can repair it later.
Every anaesthetic carries a risk, but it's very small. Modern anaesthetics are safe and your child’s anaesthetist will be an experienced doctor trained to deal with any complications.
What happens after the operation?
Children recover very quickly from grommet insertion. They should be able to go to school after a day or two.
Their hearing normally improves immediately. However, do not worry if there is still some difficulty in the first weeks, as it can take time in some cases.
Your child may have a very slight earache, which you can treat with Calpol (paracetamol).
There may be slight bleeding from their ear in the first few days following surgery. This is normal and nothing to worry about.
After an adenoidectomy.
Your child may be uncomfortable for up to a week and have a sore throat. You can treat this with Calpol (paracetamol).
Keep your child off school for 7 to 10 days. Avoid contact with anyone who has a cold or other infection, as there is a small risk of heavy bleeding from their nose. If this happens, telephone the hospital and / or go to your nearest Emergency Department.
What about swimming and grommets?
Your child must not swim for the first 2 weeks after their surgery. After 2 weeks surface swimming is allowed without earplugs. If your child wishes to dive or use water chutes, they must wear well-fitting silicone rubber earplugs.
Bath water is much worse than swimming pool water. It contains germs from the rest of the body and from soap, so do not let it get in your child’s ears. Do not allow your child to put their head under the water in the bath. For hair washing, either use earplugs or a piece of cotton wool rubbed with Vaseline. This will provide a waterproof seal.
When cleaning your child’s ears, gently clean only the outer part of their ears. Do not use cotton buds.
Will fluid discharge from my child's ear after their operation?
In the first few days after their operation, there may be a slight discharge or bleeding from your child’s ear. This is normal and nothing to worry about. After that there should be no discharge. If your child's ear continues to run and is especially smelly, that means they have an ear infection.
The infection is best treated with quinolone ear drops, which can be prescribed by your GP.
These must be inserted correctly, with your child lying on one side with their affected ear facing up.
Gently mop away the discharge.
The drops must get right into the ear canal. Massage the tragus to force the drops through the grommet into the middle ear. It is rather like plunging a blocked sink. The tragus is the piece of skin that sticks out just in front of the ear canal, like an open trapdoor.
The infection should clear up within a few days.
If your child has grommets, antibiotics taken by mouth are not very good for treating ear infections.
What happens after the grommet comes out?
The grommet only helps while it is in your child’s eardrum and open. After it has fallen out, the eardrum heals over. In 2 out of 3 cases:
the child’s hearing remains normal;
there is no further build-up of fluid; and
the condition is cured.
If the Eustachian tube is still blocked, the glue ear can come back. It may be necessary to operate again in 1 in 3 cases. Of patients who have a second set of grommets, about 1 in 3 will need a third (1 in 9 overall). Of those, 1 in 3 will need a fourth set (one in 227 overall), and so on.
Will my child have a follow-up appointment?
A follow-up hearing test will be arranged after 6 weeks. After that, we advise that your child sees their GP once a year to check their grommet is still in place.
Do grommets scar the eardrum?
Yes. But the scar does not have any noticeable effect on hearing. It is less of a problem than the scarring caused by repeated ear infections.
Contact details
If you have any queries or concerns, please contact one of the following.
Canterbury Day Surgery Centre, Kent and Canterbury Hospital, Canterbury
Telephone: 01227 783114 (7am to 8pm)Day Surgery, Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate
Telephone: 01843 234499 (Monday to Friday 7am to 9pm)
Telephone: 07887 651162 (Monday to Friday 9pm to 7am) (Bank Holidays and weekends, 24 hours a day)Channel Day Surgery, William Harvey Hospital, Ashford
Telephone: 01233 616263 (24 hours a day, 7 days a week)Dolphin Ward, Kent and Canterbury Hospital, Canterbury
Telephone: 01227 864052Padua Ward, William Harvey Hospital, Ashford
Telephone: 01233 651855
What if I have any questions or concerns?
If you have any further queries or concerns, please speak to your doctor or consultant.
Further information
References
[Web sites last accessed 28th October 2025]
Ask 3 Questions
There may be choices to make about your healthcare. Before making any decisions, make sure you get the answers to these three questions:
What are my choices?
What is good and bad about each choice?
How do I get support to help me make a decision that is right for me?
Your healthcare team needs you to tell them what is important to you. It’s all about shared decision making.
What do you think of this leaflet?
We welcome feedback, whether positive or negative, as it helps us to improve our care and services.
If you would like to give us feedback about this leaflet, please fill in our short online survey. Either scan the QR code below, or use the web link. We do not record your personal information, unless you provide contact details and would like to talk to us some more.
If you would rather talk to someone instead of filling in a survey, please call the Patient Voice Team.
Patient Voice Team
Telephone: 01227 868605
Email