Gastroscopy / PEG
Information for patients from the Trust's Endoscopy Units
This information is for patients who are having a PEG (Percutaneous Endoscopic Gastrostomy). It explains what is involved and any significant risks.
If you do not attend your appointment without telling the Endoscopy Unit in advance, you may be removed from the waiting list.
Students and trainees supervised by qualified staff may be involved in your care. If you do not want students and trainees to be present, please tell the endoscopist or nurse in charge.
The time stated is your booking in time not your procedure time. Please tell any accompanying friends or relatives.
The procedure itself takes on average 20 to 40 minutes, and may take longer if we need to carry out any treatment during the PEG. You will stay in hospital overnight. Occasionally, if there are emergency cases or very complex cases, the start of your procedure may be delayed.
What is a PEG tube?
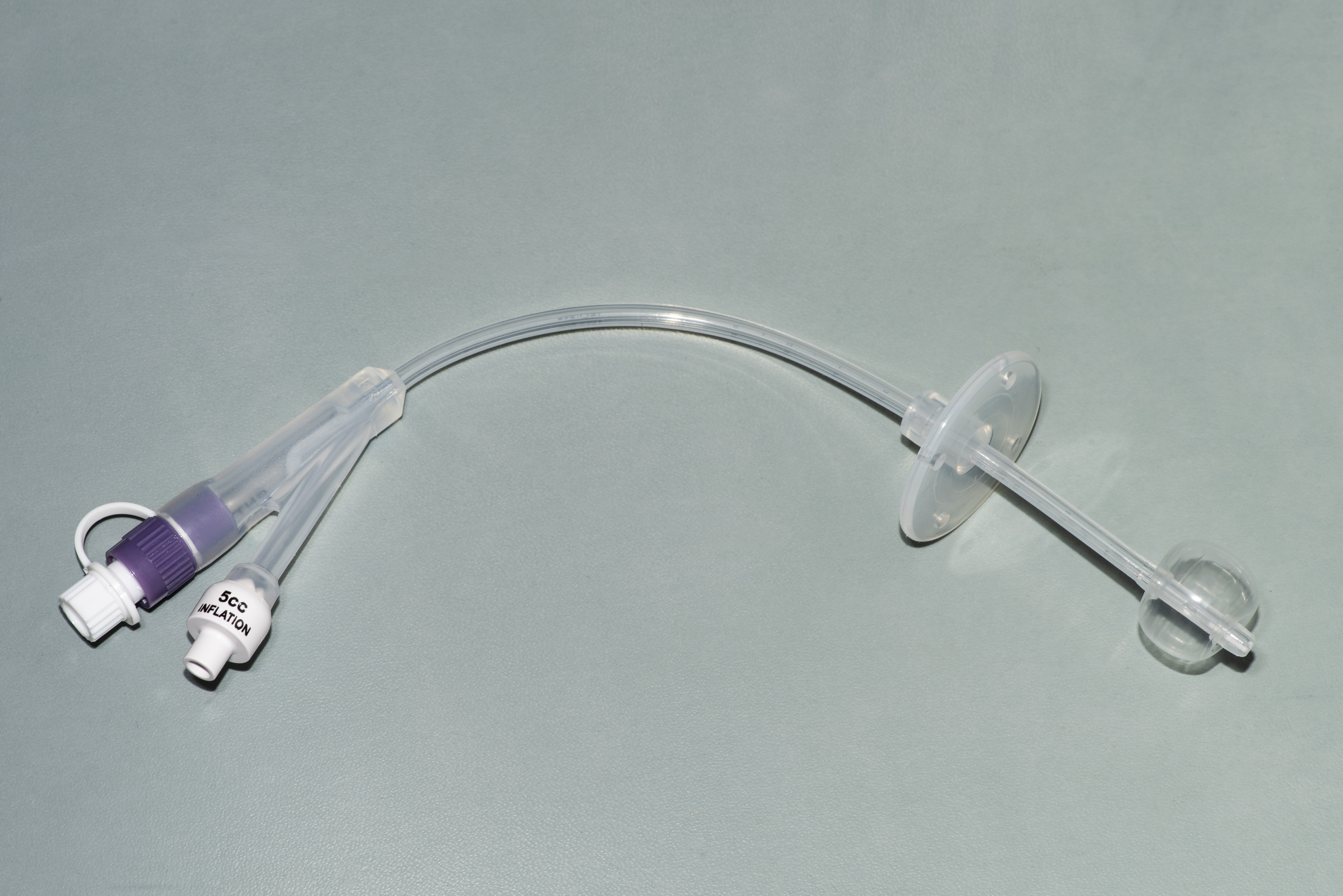
A PEG is a feeding tube inserted into the stomach using a Freka PEG tube.
To do this procedure an endoscope (a thin flexible tube with a camera at the end) is passed through your mouth, down the gullet into your stomach.
Once in the stomach a bright light will be shone showing the position of the stomach and the endoscope tip to find a suitable position to place the feeding tube.
Why do I need a PEG?
You will need a PEG if you are unable to take enough food and drink by mouth to keep your body healthy. This could be because you have had a stroke, suffer with a neurological illness such as multiple sclerosis, or receive treatments such as radiotherapy for head and neck cancer.
How do I prepare for my examination?
It is important to have nothing to eat or drink for six hours orally or by naso-gastric tube before your test.
Please bring a list of any medications you are taking.
It is especially important to remember to bring any angina sprays or asthma inhalers with you.
If you have been diagnosed with sleep apnoea and use a CPAP machine, please bring this with you to your appointment and tell the nurse on arrival.
If you are a diabetic or haemophiliac, please phone the Endoscopy Unit booked for your procedure for specific advice.
If you are taking warfarin, clopidogrel, or other blood thinning medications, please tell us at least a week before your procedure.
If you have any queries about your medication, please ring the Endoscopy Unit.
Continue to take your other medications with a sip of water.
Please remove your nail polish and all types of false nails before attending for your procedure.
Please bring with you your dressing gown, slippers, and something to do during your stay.
Do not bring any valuables to the unit. Please note that East Kent Hospitals accepts no responsibility for the loss or damage to personal property, unless the property had been handed in to Trust staff for safe-keeping.
What happens when I arrive at the hospital?
Please report to the Endoscopy Unit reception on arrival.
A nurse will check your details, blood pressure, and pulse. If you are taking any medication or are allergic to anything (medications, plasters, latex) please tell the nurse.
On the day of the PEG you will need to have a blood test to check that your blood is clotting properly.
You will be asked to remove any jewellery, spectacles, contact lenses, tongue studs, and false teeth before your procedure.
You will be given antibiotic cover about 30 minutes before your procedure to reduce the risk of infection.
You will have the procedure explained to you. You will then be asked to sign a consent form. Remember you can withdraw your consent for treatment at any time.
Please do not hesitate to ask any questions you may have.
You will need to change into a hospital gown.
A nurse will stay with you throughout your examination.
What does the procedure involve?
Your throat may be sprayed with a local anaesthetic that has a numbing affect; this has slightly a bitter taste.
A small cannula or plastic tube will be inserted into a vein, so that a sedative can be given for the procedure. This should help you feel more relaxed and sleepy. (This needle will be left lightly strapped to your hand / arm until you have recovered from the procedure).
You will be asked to lie on your left side to begin with then turned onto your back once the gastroscope has been inserted.
Then, while you are lying on your left side, a small mouthpiece will be placed in your mouth.
A small device, for recording your pulse and breathing, will be attached to your finger and you will be given oxygen.
A cuff will be placed on your arm to monitor your blood pressure (please tell the nurse if there is a reason why a certain arm cannot be used).
Once you are ready, the endoscopist will gently insert the gastroscope through your mouth and into your stomach. This is not painful and will not make breathing or swallowing difficult.
Your stomach will be gently inflated with air to expand it, so the lining can be seen more clearly. The air is sucked out at the end of the test.
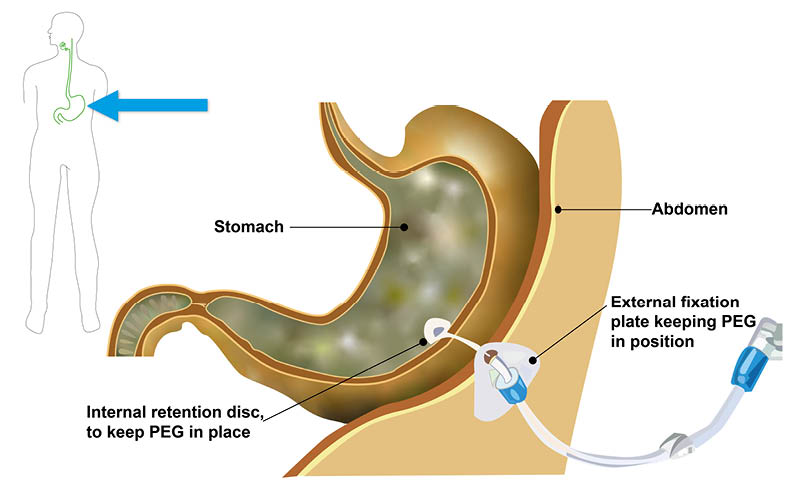
An assistant to the endoscopist will apply some local anaesthetic to your skin, then make a small incision (cut) in your abdomen wall through which a wire is inserted and pulled up through your mouth (see diagram above). The wire is attached to the PEG tube and pulled back through your mouth and into position.
A biopsy (a small sample of the stomach lining) may be taken during your examination to be sent to the laboratory for more tests. You cannot feel this.
A video recording and / or photographs may also be taken.
The nurse may need to clear saliva from your mouth using a small suction tube.
What happens after my examination?
You will return to the recovery area to rest.
You may still have a little wind but this will pass naturally.
You will stay in hospital overnight, possibly longer, to learn how to care for your PEG and to check for complications.
A letter will be sent to your GP.
You may have a mild sore throat, but this will pass and is nothing to worry about.
Are there any significant risks?
PEG placement is a generally well-tolerated procedure. The risk of complications is higher than in a gastroscopy because additional procedures are needed (for example cutting an opening in the abdominal wall). Complications are experienced by five to 10 in every 100 patients (5 to 10%).
Rarely, the condition of some patient’s may deteriorate significantly after their procedure, due to more serious complications. This happens in about three in every 100 patients (3%).
There is a risk of the following.
Damage to crowned teeth or dental bridgework.
A reaction to the sedative; the sedative can affect your breathing making it more slow and shallow.
Bleeding from the new stoma site or from one of the other organs in the abdomen.
Perforation, which is a little tear in the wall of the bowel (this is rare). If this happens you would need a short stay in hospital and treatment with antibiotics. It may need surgical repair.
Infection at the new stoma site, abdomen, or in the chest.
Failure of placement
Sometimes the stomach lies in such a position that an endoscopic gastroscopy cannot be done (this happens for approximately five in every 100 patients), so a tube cannot be inserted by the end of the procedure. Alternative techniques such as one using x-ray guidance (Radiologically Inserted Gastroscopy - RIG) or requiring open surgery and a full general anaesthetic may be necessary.
Early displacement
If the gastrostomy is pulled too hard, it can be pulled out of the stomach. The gastrostomy track may not be adequately formed for two to four weeks after PEG insertion and reinsertion of a new PEG tube may be necessary.
Please talk to your endoscopist before your examination if you have any worries about these risks.
Any further questions?
Please phone the Endoscopy Unit. The units are open Monday to Sunday 8am to 6pm.
Kent and Canterbury Hospital (K&C), Canterbury
Telephone: 01227 783058Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate
Telephone: 01843 234370William Harvey Hospital (WHH), Ashford
Telephone: 01233 616274
If you have any questions between 6pm and 8am Monday to Sunday then contact the Emergency Department on:
Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate
Telephone: 01843 235030William Harvey Hospital (WHH), Ashford
Telephone: 01233 616207
A short film outlining what patients can expect when coming to hospital for an endoscopy is available on the East Kent Hospitals web site.
If you develop any severe pain in the neck, chest, or abdomen within the first 24 hours of your procedure, please phone the Emergency Department.
Our units are regularly inspected and audited; please ask if you want any information about our performance standards. You can also visit the Care Opinion web site.