Biceps disorders / SLAP tears: labral repair
Information for patients from the Trauma and Orthopaedics (T&O) Department
You have been diagnosed with a biceps disorder or a SLAP tear. This leaflet explains what this is, the signs and symptoms, and how it can be diagnosed. Although the exact method of treatment will differ from patient to patient, the most common treatments used by East Kent Hospitals and their likely outcomes are also covered. It will also give you information about what you need to do through the process.
If after reading this leaflet you still have questions or concerns, please speak to your surgeon or anaesthetist at your next appointment.
Contents page
How does a normal shoulder work?
What is a SLAP tear?
How is the condition diagnosed?
What are the treatment options available?
What happens during my operation?
How can I prepare for surgery?
What happens on the day of my surgery?
What kind of anaesthetic will I need?
What are the complications and risks?
How long will I stay in hospital?
Will I be in pain after my surgery?
What painkillers will I be sent home with?
How do I care for my wound at home?
How long will my wound(s) take to heal?
What if my wound bleeds at home?
Can I have a bath or shower?
Why am I wearing a sling after my surgery?
What is the best position to sleep in?
When can I drive again?
When can I return to work?
When can I start my normal daily activities?
Will I have a follow-up appointment?
What if I have any questions or concerns?
Exercises and physiotherapy advice
Contact details
How does a normal shoulder work?
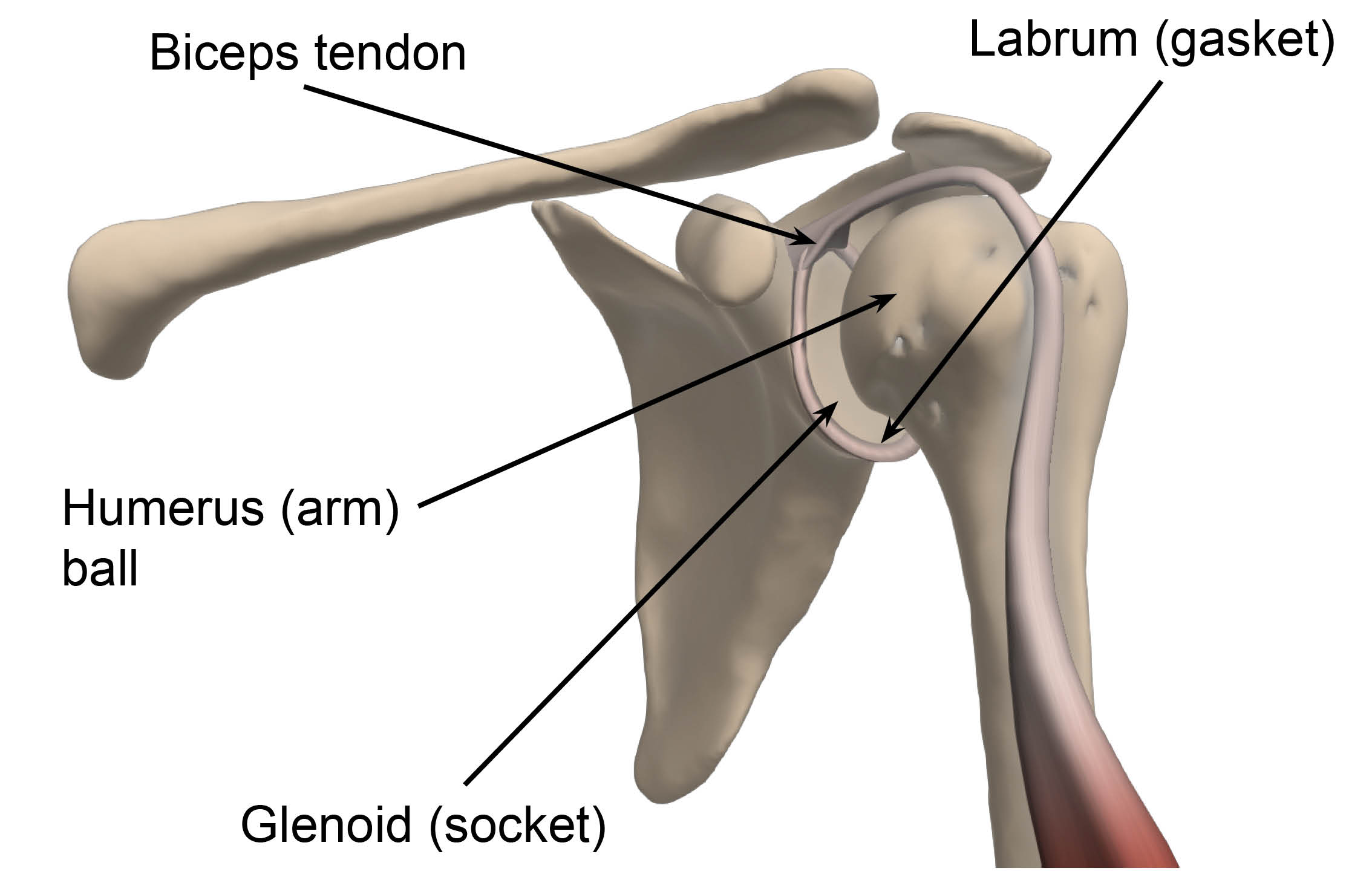
The shoulder is a ball and socket joint. The socket of the shoulder is like a flat saucer called “glenoid”, while the ball is round, called “humerus”. This allows for a large range of movement, but can make the joint unstable.
To increase the stability of the joint while allowing movement, the glenoid is surrounded by the labrum, which is a tough but flexible ring of tissue that acts like a gasket, lining and reinforcing the joint. The biceps tendon attaches to it at the top of the joint.
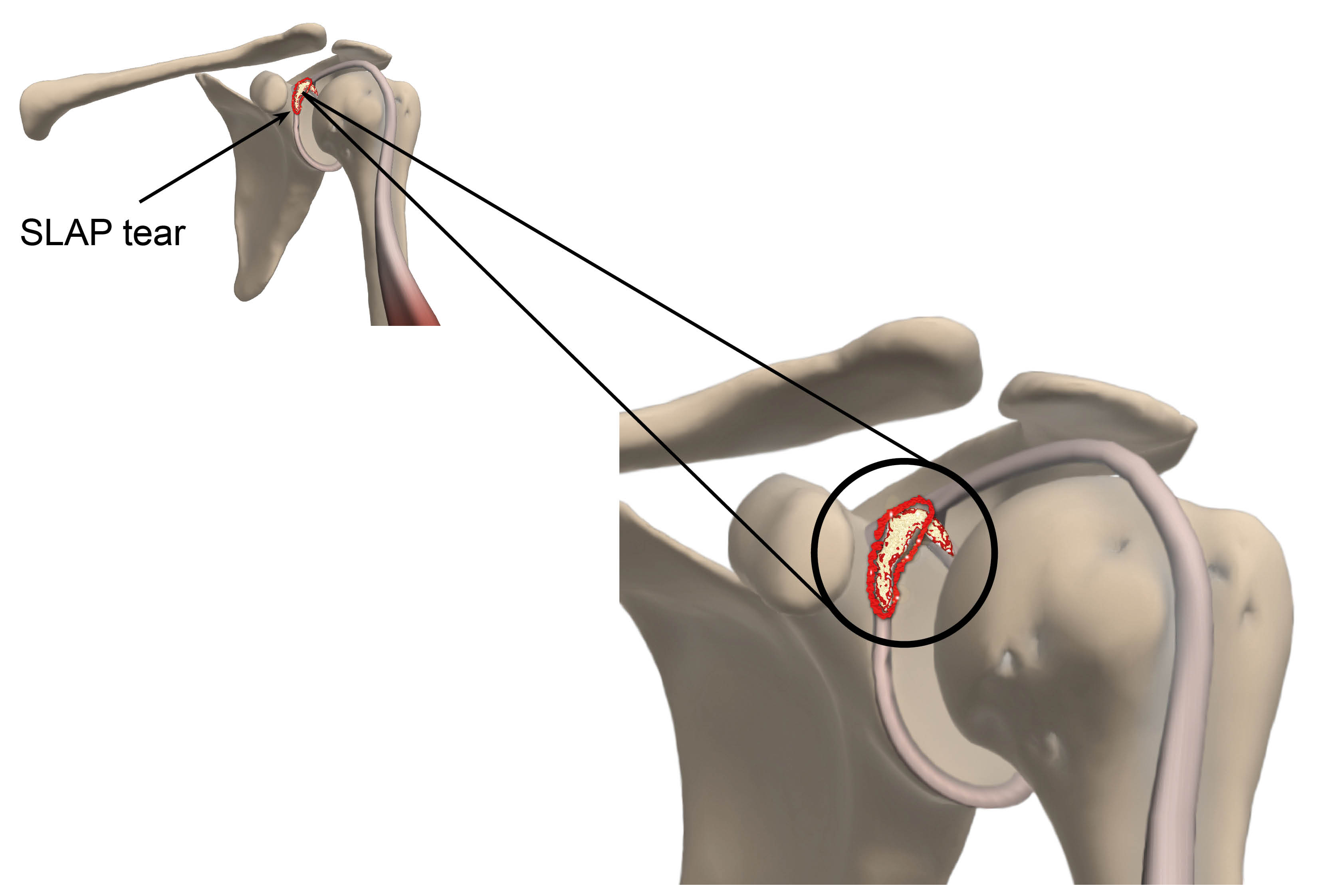
What is a SLAP tear?
A SLAP (Superior Labrum Anterior and Posterior) tear happens when the upper labrum is torn at or near its attachment with the biceps.
A SLAP tear usually happens after heavy lifting, a repeated overhead activity (such as playing tennis or throwing a ball), a shoulder dislocation, or a fall on to your outstretched hand. SLAP tears can also be a result of the wearing down of the labrum that happens slowly over time and as we age.
How is the condition diagnosed?
The diagnosis is made by physically examining the patient and discussing their medical history.
Patients may experience pain or mechanical symptoms (such as weakness) in their shoulder joint. If they have a labral tear, they may also have a history of shoulder instability or dislocations.
Magnetic Resonance Imaging (MRI) + / - Arthrogram tests can also help in confirming the diagnosis. However, if a physical examination and MRI test do not find anything, we may suggest you have a surgical procedure called arthroscopy to diagnose your condition. A diagnostic arthroscopy is a keyhole procedure that looks at your shoulder from the inside, to find out what the cause of the problem is. Any test and treatment will be discussed and agreed with you beforehand.
What are the treatment options available?
Treatment of a SLAP tear can be conservative (such as occupational therapy or physiotherapy) or surgical.
Conservative management
Most patients find that their pain settles with painkillers and / or a course of physiotherapy. Often SLAP tears are part of wear and tear in the shoulder and do not need any treatment.
Surgical management
If your shoulder continues to be painful despite simple conservative measures, then surgery can be considered to repair the tear. Surgery can be done by keyhole or open surgery. Which treatment we use for your tear will depend on the size of your tear and your general health and fitness.
Keyhole surgery is a type of operation that uses small incisions (cuts); the surgeon uses a camera and instruments to perform the surgery. Open surgery involves making a larger cut in the skin to be able to see better. The benefits of keyhole surgery is that the patient will have smaller scars and lower infection rates. In both cases and once the procedure is finished, your doctor will stitch up any incisions made and dress your wound to keep it clean and prevent infection.
All the options available to you will be discussed with you before your treatment plan is decided.
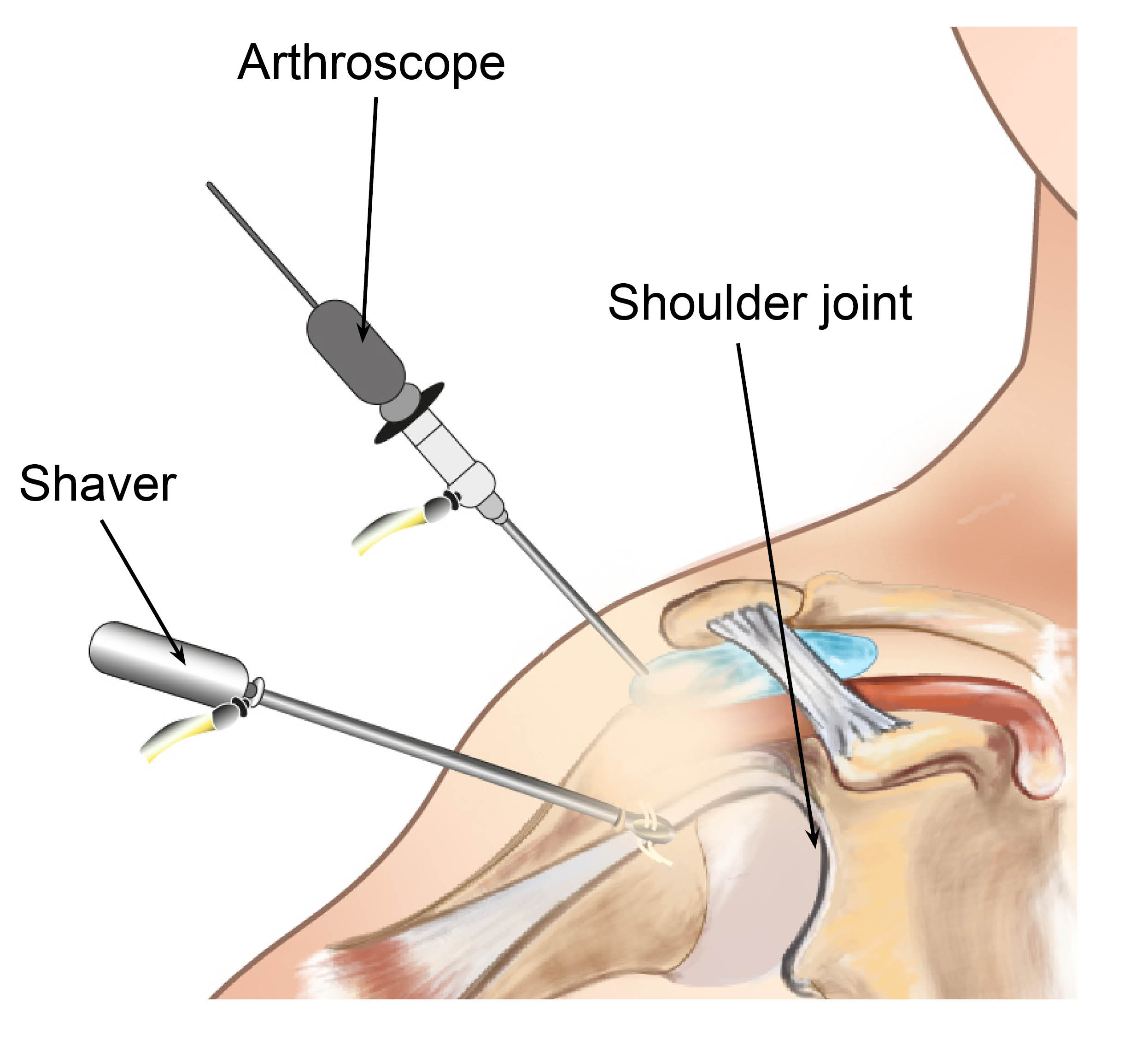
What happens during my operation?
If you are having symptoms, the tear could be treated using keyhole surgery. This means you will have three or four 5mm wounds, instead of one large one. This decreases the risk of you getting an infection during and after your surgery.
The procedure is done as a day procedure (you will be able to return home after your surgery); unless you have been told otherwise by your doctor.
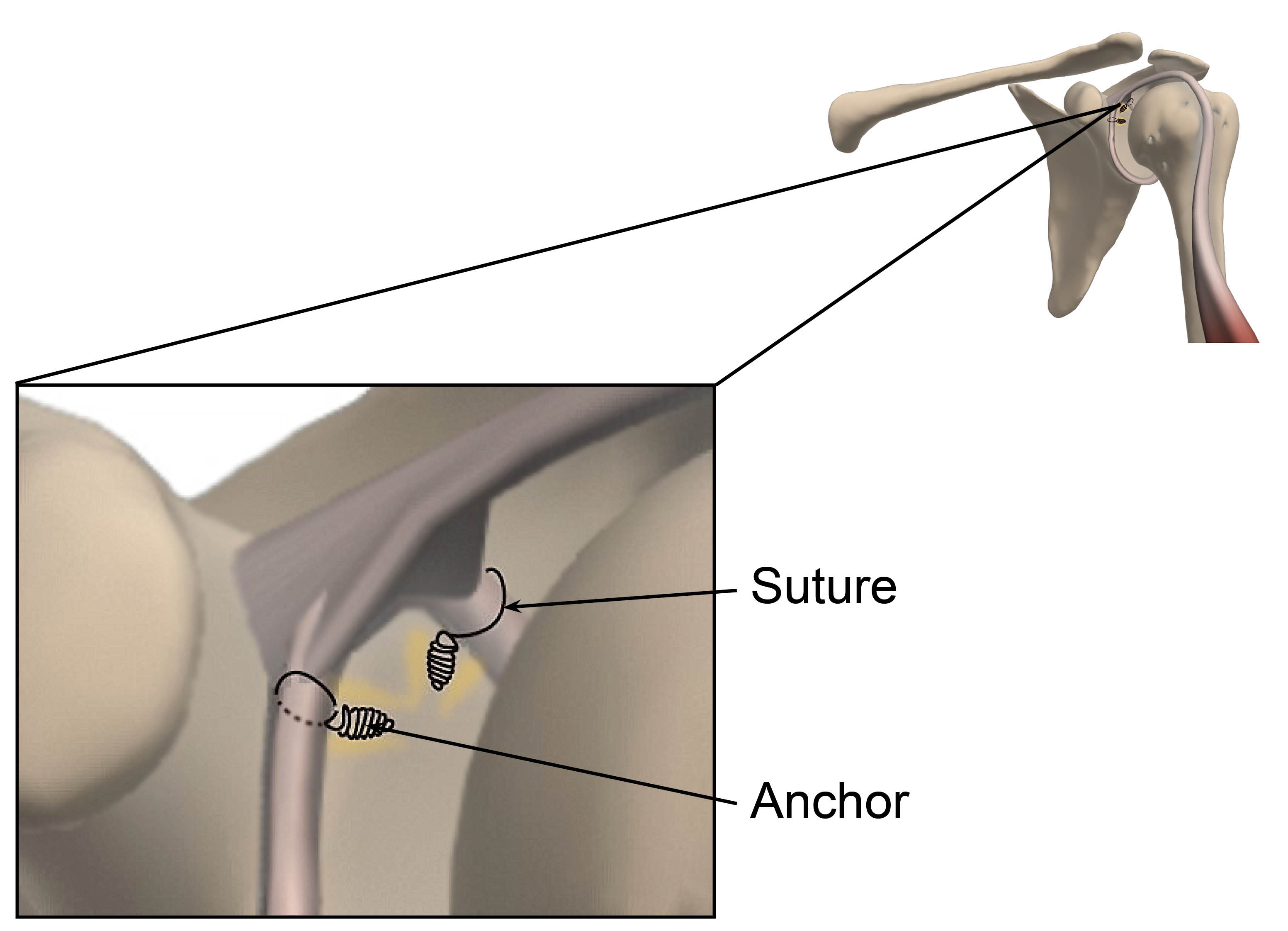
During the procedure, special bone anchors (screws) and sutures (stitches) are used to attach the torn labrum back into its normal position.
Sometimes, the tear cannot be repaired. If this happens, the injured tissue can be smoothed down (debrided) to a stable surface during surgery, which should improve your pain and shoulder function.
Your surgeon may also find further damage in your shoulder, which needs treating. This may need debridement (clean up), tendon repair, or tendon release.
It is important to keep in mind that your surgeon will not know which repair you will need until your operation is in progress. This will be discussed with you after your procedure, during your first follow-up appointment.
A doctor / physiotherapist will see you before you are sent home after your surgery. They will explain the exercises you will need to do and give you further advice to guide you through your recovery. For more information on physiotherapy and exercises, please see the end of this leaflet.
How can I prepare for surgery?
You will have a preassessment appointment before your surgery, to check if you are ready and fit for surgery. You will also be swabbed for MRSA and Covid-19, if necessary.
Before surgery it helps if you try to get as fit as possible to avoid anaesthetic risk and/or failure of the surgery. It is important that you lose weight if you are above your ideal weight.
Smoking advice
It is important to stop smoking at least 30 days before your surgery. Studies have shown that wound healing is significantly delayed by smoking / nicotine, and the infection rate is much higher. Smoking also harms how your tendon heals following a repair, so smoking after your operation is also not advised.
If you need support to stop smoking, please contact One You Kent on 0300 123 1220, or email.
How does eating a healthy diet help my recovery?
Recovering from surgery can take a long time and it is normal to get frustrated and anxious. But remember that while you are recovering, there are some things you can do to help your wound to heal. We suggest limiting the amount of alcohol you drink, stopping smoking, eating a healthy diet, drinking plenty of fluids (especially water), and staying active. If you need any extra support, do not hesitate to get in touch with us on the contact numbers listed at the end of this leaflet.
Some painkillers (especially those containing Codeine) can cause constipation. To avoid this, please follow a healthy well-balanced diet rich in fruit, vegetables (including green leafy vegetables), nuts, seeds, wholegrains, and legumes, which contain the necessary fibre, and drink plenty of water. More information is available on the NHS 5 A Day: what counts? web site.
While you wait for your surgery date, you can start preparing for your operation. Research shows that fitter patients, who are able to improve their health and activity levels before surgery, recover more quickly. Taking an active role in planning and preparing for your operation will help you:
feel in control
leave hospital sooner, and
get back to normal more quickly.
To help with this, you may be contacted by a member of the One You Kent (OYK) team. OYK work in the community, and help patients improve their general health. This includes help and advice on:
Stopping smoking
Losing weight
Getting more exercise
More information can be found on the following web sites.
One You Kent (Kent Community Health)
Fitter Better Sooner Toolkit (Royal College of Anaesthetists)
What happens on the day of my surgery?
Please arrange for someone to pick you up from the hospital after your surgery, as you will not be able to drive yourself. Please make sure to arrange this before your surgery.
To avoid complications with your anaesthetic, you should not eat anything for six hours before your surgery, or drink anything for two hours. You will be given further instructions during your preassessment.
On the day of your surgery, you can take your usual medication as advised during your preassessment. If possible, do not take non-steroidal anti-inflammatory medication, such as ibuprofen and naproxen, for at least 10 days before your surgery, as they can affect how your wound heals. Please bring any medications that you are taking into the hospital with you.
If possible, please wear loose-fitting clothes, as after surgery you will be wearing a sling.
Bring your appointment letter with you, so you know which department to come to when you arrive at the hospital.
At arrival, you will be asked to put a hospital gown on, and maybe a pair of compression stockings.
You will see the anaesthetic and surgical team before your surgery to go through the consent form and discuss any questions you may still have. Remember you can withdraw your consent for treatment at any time.
You may be tested for Covid-19. All appropriate precautions will be taken during your admission to minimise the risk of contracting the illness as per Healthcare England Guidelines.
What kind of anaesthetic will I need?
This procedure is usually performed under general anaesthetic (you will be asleep for the procedure). However, you may be offered the option of “awake anaesthesia” during your surgery to avoid putting a tube into your windpipe. This may be discussed and decided with you and the anaesthetist on the day of your surgery. Should you be suitable for this type of anaesthesia, it is important to understand and be assured that you will be kept comfortable, and you will not feel any pain during your procedure. Patients describe their experience after this type of “awake anaesthetic” as if waking up from a usual night’s sleep, as it is often supplemented with some light sedation. If you need any more information, please speak to your anaesthetist before your procedure.
In addition, a local anaesthetic or nerve block is used during your operation. As a result, your shoulder and arm may feel numb for a few hours after your operation. It is important to take your pain medications during this time, to allow a gentle and easier control of pain when the nerve block wears off and your shoulder is likely to be sore and uncomfortable.
What are the complications and risks?
As with all surgery, there are a few risks and complications with shoulder surgery. These are rare and will be discussed with you before your surgery.
The risks to having this surgery include the following.
Wound infection: we do everything we can to avoid this but an infection might still happen. If your wound becomes increasingly red or swollen after your surgery, please contact your GP or speak to your surgical team.
Local swelling could happen due to the surgery “upsetting” the soft tissues around your elbow, but it should improve as you recover from your surgery.
Bleeding: if this happens during your surgery, we will do our best to stop it as soon as possible. However, some oozing could still happen after your surgery. For more information, see the What if my wound bleeds at home? section below.
Soft tissue (nerve / tendon / blood vessel) injury could happen during surgery. If this happens, your surgeon will try to deal with it during your operation and it will be discussed with you after your surgery.
The bones of the shoulder may fracture; this is because of the force used while performing the surgery. We will do our best to avoid this happening.
Prolonged stiffness and or pain / frozen shoulder, that may cause frozen shoulder (your shoulder is painful and stiff for up to several months beyond the usual period expected for the stiffness to recover from a simple procedure). This could be avoided or improved if you take adequate pain relief and do the exercises listed at the end of this leaflet as your pain permits.
Deep vein thrombosis (DVT) and / or pulmonary embolism (PE). These are blood clots which form in the blood stream and can be serious conditions. Compression stockings and other measures might be taken by the hospital to avoid them.
Sometimes symptoms may persist and you may need further treatment, if appropriate.
If the result is unsuccessful or the repair fails, we may need to repeat the surgery.
Complications relating to the anaesthetic. You will speak to your anaesthetist before your surgery, and they will explain these to you.
If you have any questions or concerns about these complications, please speak to your doctor either during your clinic appointment or before your surgery.
How long will I stay in hospital?
This procedure is usually carried out as a day operation, so you should be able to go home the same day.
After your operation, you will be taken to the ward until it is safe for you to be discharged home. You will be seen by your surgeon, surgical care practitioner, and / or physiotherapist before you go home. They will show you exercises to do and give further advice to guide you through your recovery.
If you need to stay in hospital overnight, this will usually be explained to you during your preassessment appointment. If you have to stay overnight, make sure you bring with you items you may need, such as hygiene items (toothpaste and toothbrush), a dressing gown, slippers, and your usual medication. Also, we suggest you bring a book or magazine, in case there is a delay.
Will I be in pain after my surgery?
This type of surgery may be uncomfortable, and you will need appropriate pain relief afterwards. If your anaesthetist has given you a nerve block, your shoulder and arm may feel numb and weak. You may not feel any pain immediately after your surgery, as the block may take 12 to 24 hours to wear off completely.
However, it is very important that you take your pain relief as advised and as early as you can before the nerve block wears off; this will help you to keep on top of your discomfort. It is advisable to take your painkillers regularly for the first few days. If possible, avoid non-steroidal anti-inflammatory medication, such as ibuprofen and naproxen, for at least 10 days before your surgery and six weeks following surgery. This is because anti-inflammatory medication could slow down the healing process.
You will be given painkillers when you leave the hospital, to take at home; these should last for at least two weeks. This will be discussed with you before you leave hospital.
Take pain relief regularly to try and keep your level of discomfort at a bearable level at all times. This allows the inflammation (redness, swelling, and heat) and pain to settle. Do not wait until your shoulder is very painful to take the pain relief, as it is then more difficult to control.
What painkillers will I be sent home with?
Surgical patients might be given some of the following painkillers, depending on their age, body weight, and individual circumstances, unless told otherwise by their doctor.
Take each painkiller as advised on your prescription.
Tablet paracetamol, 1g every four to six hours (no more than 4g per day).
Codeine Phosphate, 30 to 60mg every six to eight hours.
Tablet Tramadol, 50 to 100mg every eight hours.
Oramorph, 10 to 20mg every hour, as needed.
Please note that Codeine, Oramorph, and Tramadol should not be taken together; you should only take one of the three at any one given time.
Ice packs or bags of frozen peas may also help reduce your pain. Wrap the pack / bag with a cloth and place it on your shoulder for up to 15 minutes. Do not eat these peas for once they have defrosted.
If your pain continues and is not controlled with the medication you have been advised to take, then please contact your GP. You may also contact the East Kent Upper Limb Team if you need further help.
If you notice your wound area is becoming more painful, red, hot, and / or discharging pus (thick yellow discharge), you may be developing an infection. Contact your GP or your surgical team for advice as soon as possible.
How do I care for my wound(s) at home?
If you had a repair through keyhole surgery, there will be few (three to five) wounds.
It is important to keep your wound and dressing dry and in place until your wound is well healed, and have your stitches removed at your two week follow-up appointment with your GP practice nurse or at the hospital, with your surgeon or your nurse practitioner (surgical care practitioner). You will be told where your follow-up appointment is going to be before you leave the hospital.
If the dressing gets wet or bloodstained, you can change them yourself by carefully placing a dressing from a pharmacy. If you are unable or have difficulties doing this yourself, you can ask a relative or a friend to change it for you, or you can make an appointment with your GP practice nurse to do it for you.
If you are being seen by your GP practice nurse for a wound check 10 to 14 days after your surgery, please make sure the nurse reads the following. These instructions are for healthy looking surgical wounds only.
*Colourful stitches are non-absorbable and need to be completely removed to avoid them getting buried under the patient’s skin.
*White / clear stitches are absorbable. If any suture knots have been made outside the patient’s skin, please remove these to avoid suture abscesses. Thank you.
*The appearance and material of the sutures can be different from Trust to Trust, but these are the most common.
If a wound does not seem to be healing appropriately, please leave the stitches / knots in place and make another appointment to remove them in few days.
How long will my wound(s) take to heal?
Wounds usually take between 10 to 14 days to heal.
The area around your wound(s) may have some numbness, which is usually temporary. You may feel occasional sharp pains or ‘twinges’, as well as itching near the scar as it settles.
What if my wound bleeds at home?
Occasionally there can be minor bleeding or clear fluid ooze in the first day or two after your surgery. If your dressings get wet or bloodstained, you can change them yourself by carefully placing a dressing from a pharmacy over your wound. If you are unable to this yourself, you can ask a relative or a friend to help or you can get an appointment with your GP practice nurse to do it for you. This bleeding or oozing should be controlled by pressing firmly but gently on your wound for 15 minutes.
If you are worried about the bleeding, you can contact the hospital on the number given to you (during normal working hours) or go to a walk-in centre or Emergency Department (after hours).
Can I have a bath or shower?
You should have a ‘dry wash’ or a shallow bath instead of a shower. This keeps your arm in the correct position and prevents your dressing(s) and sling from becoming wet.
While your wound is still healing:
do not use soaps, lotions, creams, or powders on your wounds, to avoid any infection getting in to your wound(s); and
keep your wound(s) dry at all times.
It is very important to remember to keep your armpit on your operated side clean and dry. Lean forward so you can reach your armpit, as separating it from the body sideways may be difficult or painful and is not allowed for the first four to six weeks.
You can wash and clean the area as normal once your wound is completely healed.
Why am I wearing a sling after my surgery?
You will return from surgery wearing a sling. This is usually used for the first four to six weeks following your operation. The sling protects your tendon repair while it heals. At the beginning, you can only remove your sling to exercise, wash, and dress. Do you remove the sling for anything else, unless told otherwise by your surgeon or physiotherapist.
While wearing the sling, you may find that your armpit becomes uncomfortable. If you lean forward you will be able to reach your armpit and use a dry pad or cloth to absorb any moisture.
As you begin to heal you will be able to slowly stop using your sling. Your physiotherapist will advise you about this. To start with you can remove your sling when sitting watching TV or reading, and just rest your arm by your side or on cushions. Do not remove your sling unless you have been told to by your surgeon or physiotherapist.
You should avoid forcing your elbow to straighten or heavy lifting for at least six weeks after your surgery.
After three months your symptoms should improve, but patients rarely get all their movement back. Your shoulder may take six months to totally settle.
What is the best position to sleep in?
To begin with sleeping will be difficult. Take regular painkillers and try to support your shoulder with pillows, by placing them behind it. If you lie on your back, a pillow under your arm and elbow may make you feel more comfortable. You may also find it easy to lay on your non-operated side.
You can lay on your operated shoulder once you feel comfortable to do so.
When can I drive again?
You will not be able to drive for at least six weeks following your surgery. Your surgeon will tell you when you can drive again. The advice from the DVLA is that you should not drive until you are physically capable of controlling a motor vehicle and can perform an emergency manoeuvre, such as an emergency stop.
Please arrange for someone to collect you from hospital and take you home after your surgery.
When can I return to work?
This will depend on your job. Your surgeon will advise you on the amount of time you will need to be away from work; you can ask for a sick note before you leave the hospital. If you have an office job or light duties, you can return to work as soon as you feel able to. If you have a job that needs you to lift heavy objects or one that involves using your arm above shoulder height, you will not be able to do this until at least eight weeks after your surgery.
When can I start my normal daily activities?
You should avoid repetitive activities where you need to move your arm above shoulder height, or activities where you have to force your elbow to fully extend for three months; this includes tennis, golf, or swimming, as well as contact sports. For advice on DIY and racquet sports you should speak with your physiotherapist.
Will I have a follow-up appointment?
You will be seen by your surgical care practitioner or your surgeon two to six weeks after your surgery. They will check your progress, make sure you are moving your arm correctly, and give you further instructions and exercises as appropriate.
An appointment will be made for you to see a physiotherapist after your discharge from hospital. This appointment will usually be three to four weeks after your surgery. You will be monitored by a physiotherapist throughout your rehabilitation.
What if I have any questions or concerns?
If you have any questions or concerns, please contact your surgical care practitioner, surgeon, or physiotherapist. Their contact details are listed at the end of this leaflet.
If you notice your wound area is becoming more painful, red, hot, and / or discharging pus (thick yellow discharge) you may be developing an infection. Contact your GP or your surgical team for advice as soon as possible.
Exercises
The following are basic exercises that all patients can do, as their pain allows; do not do them if they hurt. These exercises are a guide, your physiotherapist will give you further advice on this before or after your surgery.
Physiotherapy guidelines while you are still in the hospital
A follow-up appointment to see the physiotherapy team will be made for you before you leave hospital. This appointment will be within three weeks of your surgery, unless you are told otherwise by the physiotherapy team.
How to manage your sling will also be explained before you leave hospital. Including how to take it on and off and keep it clean and clear of infection.
You will be shown how to do the following exercises on the ward
elbow, wrist, and hand exercises
shoulder girdle and posture exercises
pendular shoulder exercises
assisted movements into shoulder flexion and assisted movements into external rotation of your shoulder within the “safe zone” as dictated by your surgeon in your operation notes. A relative/friend can be taught these as well.
Physiotherapy guidelines once you leave the hospital
Your outpatient physiotherapy will start within three weeks of your surgery, unless you are told otherwise. Until then, you can start doing the following exercises as your pain allows. Any questions can be discussed with your physiotherapist before or after your surgery, or by calling one of the physiotherapists listed at the end of this leaflet.
Early exercises: you can do these three times a day.
Hand exercises
Open and close your fist 20 times.
Wrist exercises
Move your wrist up and down 20 times.
Forearm exercises
Turn your palm up and down 20 times.
Elbow exercises
Bend and straighten your elbow 20 times. This can be completed with help from your other arm.
Shoulder girdle and posture
Try not to slouch after your surgery.
Try pulling your shoulder blades back and down 20 times.
Pendular exercises
Lean forwards, supporting yourself with your other arm.
Swing your operated arm forwards and backwards gently, similar to a pendulum.
Do this 20 times.
You will be shown further exercises at your outpatient physiotherapy appointment or your clinic appointment. If you have any questions, please contact the physiotherapists listed in the contact details below.
Contact details
Consultants and their secretaries
The teams listed below work at Kent and Canterbury Hospital as well.
| Hospital site | Consultant | Secretary name | Contact number |
|---|---|---|---|
| Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate | Mr Sathya Murthy | Tracy Blackman | 01843 235068 |
| Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate | Mr Georgios Arealis | Donna Cannon | 01843 235083 |
| William Harvey Hospital, Ashford | Mr Paolo Consigliere | Heather Littlejohn | 01233 616280 |
| William Harvey Hospital, Ashford | Mr Jai Relwani | Dione Allen | 01233 616737 |
| William Harvey Hospital, Ashford | Surgical Care Practitioner | Alphonsa Augustine | 07929 375381 |
Physiotherapists
| Hospital site | Physiotherapist | Contact number |
|---|---|---|
| Buckland Hospital, Dover | Abi Lipinski | 01304 222659 |
| Kent and Canterbury Hospital, Canterbury | Sarah Gillet (inpatient) | 01227 866365 |
| Kent and Canterbury Hospital, Canterbury | Darren Base | 01227 783065 |
| Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate | Caroline Phillipott (inpatient) | 01843 234575 |
| Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate | Martin Creasey | 01843 235096 |
| Royal Victoria Hospital, Folkestone | Ailsa Sutherland | 01303 854410 |
| William Harvey Hospital, Ashford | Cindy Gabett (inpatient) | 01233 633331 |
| William Harvey Hospital, Ashford | Chris Watts | 01233 616085 |
Surgical Preassessment Units
| Hospital site | Contact number |
|---|---|
| Kent and Canterbury Hospital, Canterbury | 01227 783114 |
| Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate | 01843 235115 |
| William Harvey Hospital, Ashford | 01233 616743 |
Fracture Clinics
| Hospital site | Contact number |
|---|---|
| Kent and Canterbury Hospital, Canterbury | 01227 783075 |
| Queen Elizabeth the Queen Mother (QEQM) Hospital, Margate | 01843 235056 |
| William Harvey Hospital, Ashford | 01233 616849 |