Arthritis of the big toe (Hallux Rigidus)
Information for patients from Trauma and Orthopaedics (T&O)
You have been referred to the hospital as you have arthritis in your big toe. This leaflet explains:
what causes big toe arthritis
what the treatment options are
what the risks are to having surgery; and
what happens if you choose not to have surgery.
We hope this leaflet helps to answer some of the questions you may have. If you have any further questions or concerns, please speak to a member of your healthcare team.
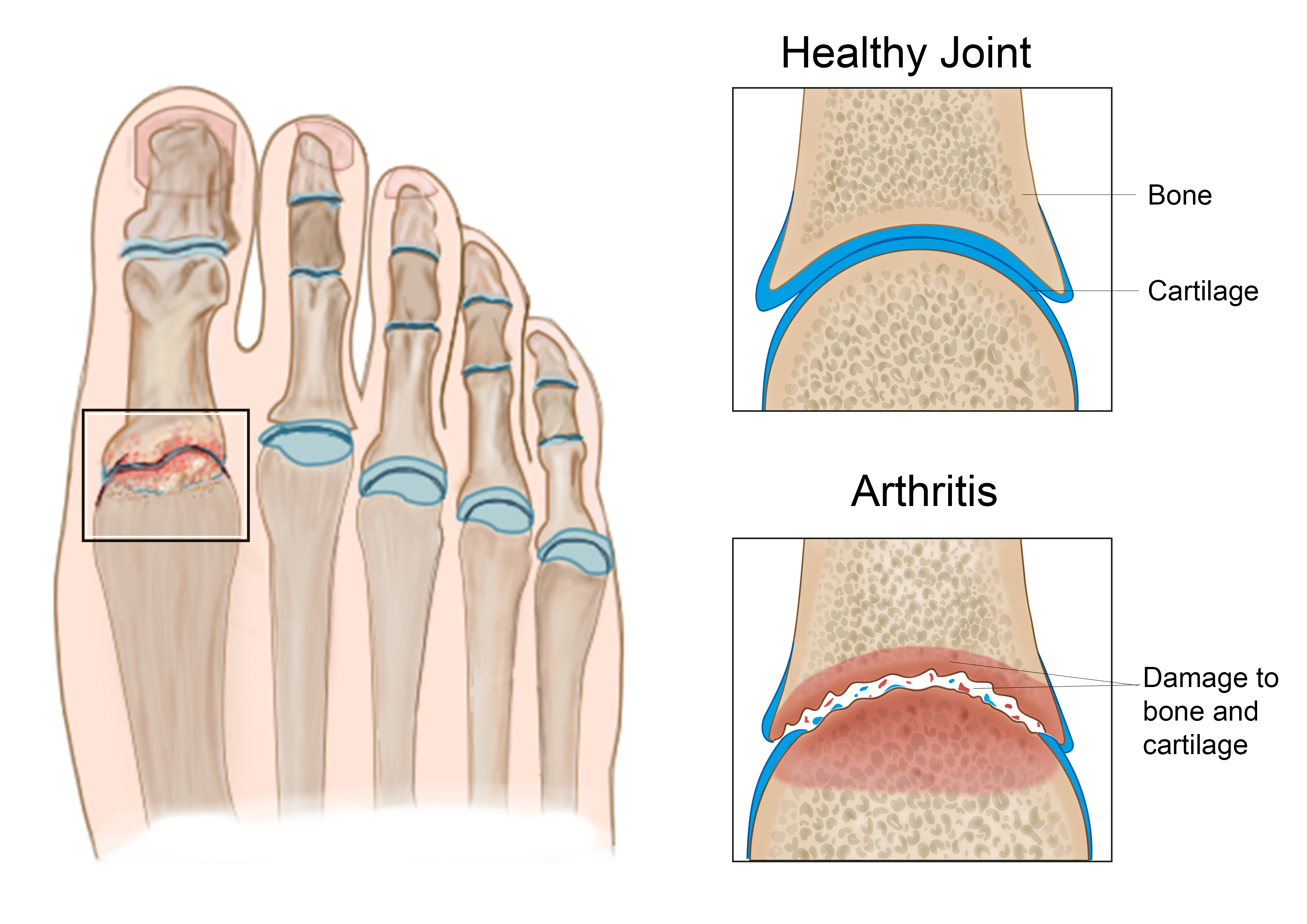
What is Hallux Rigidus?
Hallux Rigidus happens when your toe joints become rigid due to arthritis. This causes pain and swelling. Arthritis happens when the lining of the bones in your joint become damaged.
What causes Hallux Rigidus?
Arthritis of the big toe may happen:
following infection or trauma (an injury)
after an episode of gout; or
from inflammatory arthritis / osteoarthritis.
What are the treatment options?
To help with pain and swelling you can take:
painkillers (such as paracetamol and ibuprofen); and
non-steroidal inflammatory medication.
In the earlier stages of arthritis, a steroid injection into the joint may help.
Making changes to your footwear may also help. For example:
a soft shoe with a toe box will relieve pressure on your toe; and
a stiff-sole or rocker-bottom shoe will relieve your pain by reducing joint movement.
You should only consider surgery after you have tried the treatment options listed above.
What surgical options are available?
In the early stages of arthritis, the main issue is pain from the osteophytes (bone spurs) rather than from general arthritic pain. To help with this, there is an option to remove the osteophytes (cheilectomy) and keep the joint. If this is not successful, you may need a fusion procedure.
In more advanced arthritis, fusion is thought to be the best option. During this procedure, the surgeon will make an incision (cut) on the top of your toe and join the bones on either side of your joint together. This is usually held together with either screws, plates, or a combination of both. Once healed, the joint remains stiff and the pain goes, as the joint surfaces no longer rub on each other.
In some cases, particularly with patients who do not move around much, we can consider a silastic joint replacement. However, there is no long-term evidence to support this treatment.
You will discuss these procedures with your surgeon, before any decisions are made about treatment. Your surgeon will discuss which procedure is more appropriate for your condition. Please use this time to ask any questions or raise any concerns you may have.
Will I have a general anaesthetic?
Most patients have a general anaesthetic (you are asleep for the procedure).
What happens if I ignore my condition?
The reason(s) why you came to the appointment may not get better and sometimes can get worse. It is difficult to predict.
How long will I have to stay in hospital?
This surgery is usually performed as a day case procedure (you can go home on the same day). However, if you have a fusion procedure you may need to stay in hospital overnight.
You will need someone to drive you home after your surgery, and someone must stay with you overnight.
How can I prepare for my surgery?
The nurse at your pre-assessment appointment will tell you:
when to stop eating / drinking before your surgery,
what to do with your medications; and
where to come on the day of your surgery.
While you wait for your surgery date, you can start preparing for your operation. Research shows that fitter patients, who are able to improve their health and activity levels before surgery, recover more quickly. Taking an active role in planning and preparing for your operation will help you:
feel in control
leave hospital sooner; and
get back to normal more quickly.
To help with this, you may be contacted by a member of the One You Kent (OYK) team. OYK work in the community, and help patients improve their general health. This includes help and advice on:
Stopping smoking
Losing weight
Getting more exercise
More information can be found on the following web sites.
One You Kent (Kent Community Health)
Fitter Better Sooner Toolkit (Royal College of Anaesthetists)
What happens when I arrive at the hospital?
When you arrive at the hospital you will be seen by the nurses, a physiotherapist, and doctors who will explain your procedure. Please use this time to ask any questions.
You will be asked to change into a hospital gown and stockings.
.png)
What happens after my surgery?
After surgery you will have a bandage on your ankle.
You will also be wearing a surgical boot. The boot allows you to put weight on your affected leg whilst protecting your foot. Unless your surgeon has told you otherwise.
One of your healthcare team will give you crutches for support. Please use these as advised by your doctor.
Elevate (raise) your ankle as much as possible in the first few weeks after your surgery. Move your ankle as much as possible as well.
Everyone reacts to the general anaesthetic differently. Feeling sick is common and we do our best to avoid this.
Will I have a follow-up appointment?
Yes. You should have your wound checked in clinic two weeks after your surgery. If you had fusion surgery you will have another appointment at six weeks, when we will take an x-ray of your toe.
When will my bandages be removed?
Your bandages will be removed at your two week clinic appointment and your dressings changed.
When can I stop wearing my surgical shoe?
If you had joint replacement surgery, the surgical shoe can be removed at your two week appointment. You can start to wear a normal comfortable shoe instead (often a size up from your normal size).
If you had fusion surgery, you will need to keep wearing the surgical shoe when you put weight on your toe for approximately five to six weeks.
Will I need physiotherapy after my surgery?
A physiotherapist will see you after your surgery, to make sure you are safe in your surgical shoe and crutches. You should not need any further physiotherapy, but an appointment can be made if needed.
When can I start driving again?
This is a difficult question to answer. Your healthcare professionals are not able to take responsibility for this.
You will need to check with your insurance company about when they will be willing to insure you to drive again. You must not be in a cast or boot when driving. You must be able to do an emergency stop safely before driving again.
When can I return to work?
When you can return to work depends on how much your work needs you to put weight on your affected toe. If you sit down a lot and can keep your foot elevated, you can return to work after two weeks. If this is not possible, and your job is more active, you can expect to return to work after four weeks.
What are the risks?
As with any surgery there are risks. Your surgeon will discuss these with you in more detail before your procedure.
Common complications of this type of surgery include the following.
You can expect swelling for up to 12 months, particularly in the evenings.
The position of your ankle and foot may not be satisfactory after fusion. Although this is rare, it can be significant if it does happen. You may need further surgery.
Infection rates are low, and antibiotics are given before any surgery. If you do develop an infection, this can cause problems.
A skin infection can be managed with antibiotics.
If you develop a deep infection, we may need to remove all the metalwork and unhealthy bone. You will also need a long course of antibiotics. In the case of ankle replacements, a repeat of the procedure may be necessary to correct the problem.
Nerve injury can result in numbness or tingling across your foot area. This is usually temporary, but in a small number of cases it may become permanent.
Non-union can sometimes happen with fusion surgery. Non-union is when the bones do not join together successfully. There is more risk of this happening in smokers. It may result in pain if the metalwork then loosens. If you smoke, stop before surgery and do not start again until the fusion has healed.
If you need support to stop smoking, please contact One You Kent on 0300 123 1220, or email.
Although rare, metalwork can become noticeable through your skin. This can cause pain from irritation. If this continues we may need to remove the metalwork.
Complex Regional Pain Syndrome (CRPS) can develop when the nerves around the operation site become overly sensitive. Swelling, skin changes, and stiffness can happen and can be debilitating. This is rare, but if it does happen it is usually managed by a specialist in pain management.
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) is rare with this surgery. Anticoagulation medication is given after surgery, to try to prevent clots forming whilst you are not able to move your leg. This is a preventative measure, but a clot can still form.
If you have any concerns or questions about any of these risks, please speak with your doctor before your surgery.
What if I have any questions or concerns once I return home?
If you have any questions before your surgery, contact the team secretary through the hospital switchboard.
After surgery you can call the team secretary, the ward, or your GP if you have any further concerns or questions. If you have concerns and cannot get in touch with anyone, go to your nearest Emergency Department.
Ask 3 Questions
There may be choices to make about your healthcare. Before making any decisions, make sure you get the answers to these three questions:
What are my choices?
What is good and bad about each choice?
How do I get support to help me make a decision that is right for me?
Your healthcare team needs you to tell them what is important to you. It’s all about shared decision making.
What do you think of this leaflet?
We welcome feedback, whether positive or negative, as it helps us to improve our care and services.
If you would like to give us feedback about this leaflet, please fill in our short online survey. Either scan the QR code below, or use the web link. We do not record your personal information, unless you provide contact details and would like to talk to us some more.
If you would rather talk to someone instead of filling in a survey, please call the Patient Voice Team.
Patient Voice Team
Telephone: 01227 868605
Email